The intent of this document is to educate end users about the Inventory Management Workflow for completing the immunization task.
The system attempts to find an existing lot when scanning or manually searching for a lot – both workflows pull information from the MPage/Inventory Mgmt. Worklist when charting an immunization in Medication Administration Record (MAR).
Task List Workflow:
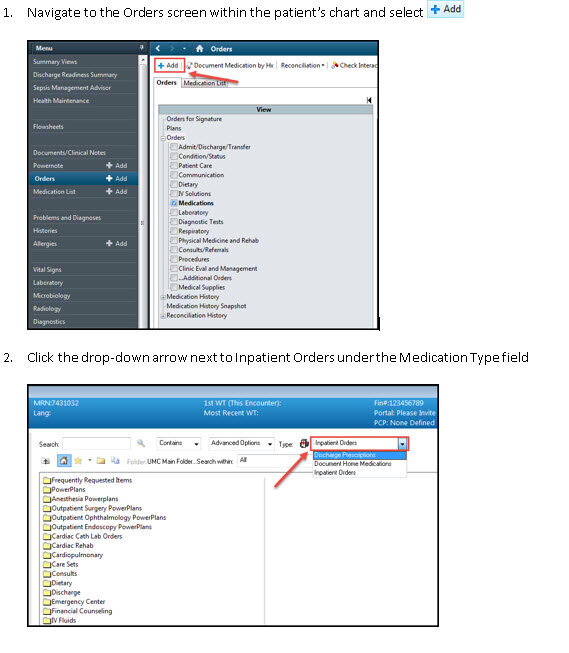
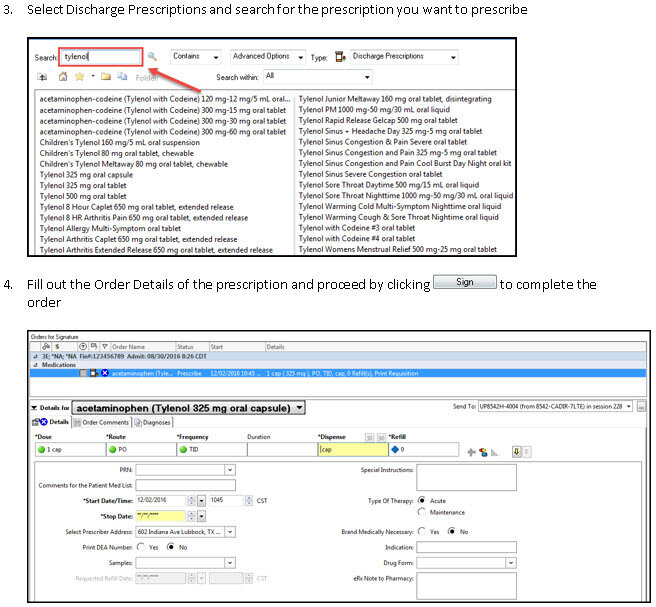
From the Multi-patient Task List (MPTL), select the patient which the immunization was ordered, OR from the Patient Task List select the immunization medication that is being adminstered
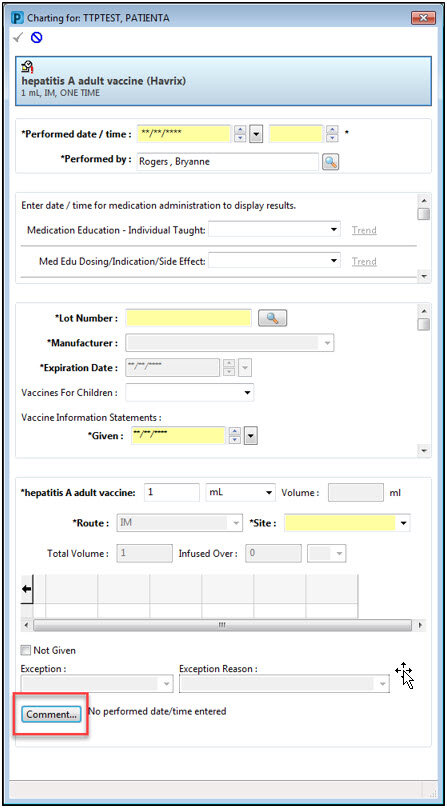
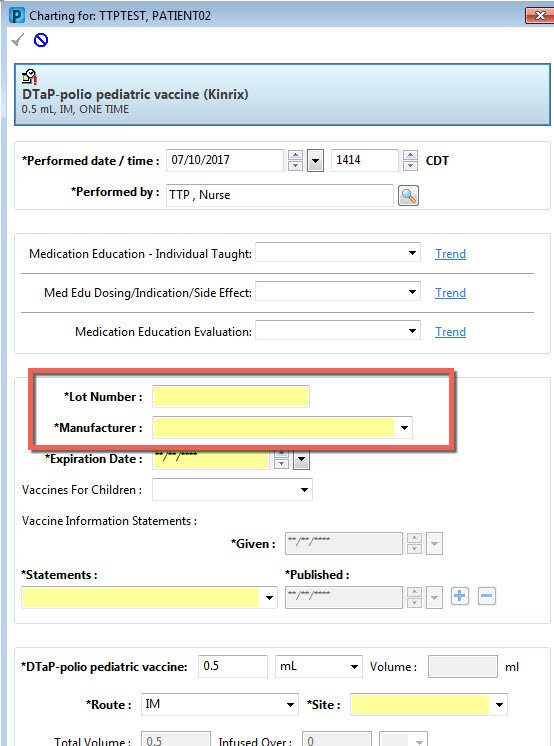
The administration window will appear with the Lot # field yellow and the maunfaturer and expiration date dithered:

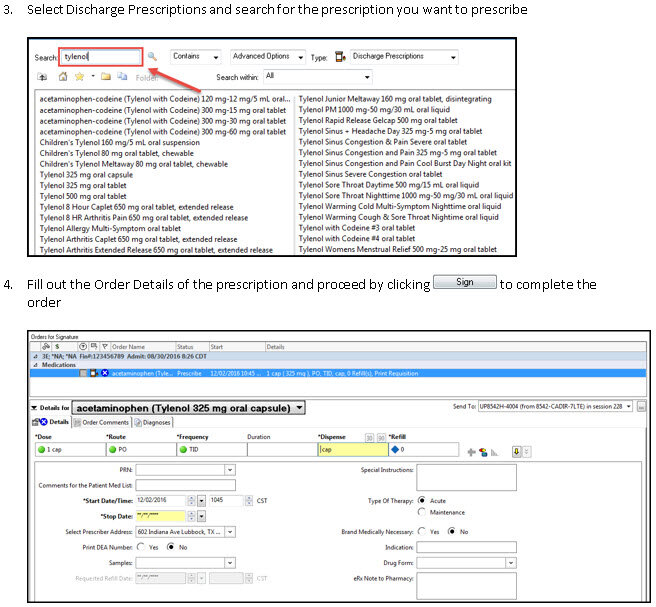
Enter the lot # and select the magnifying glass search icon
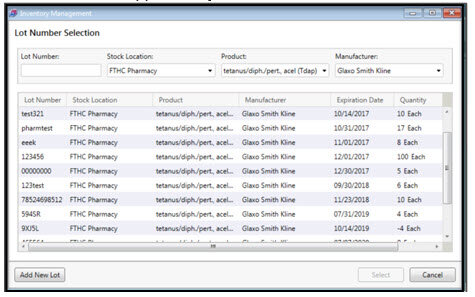
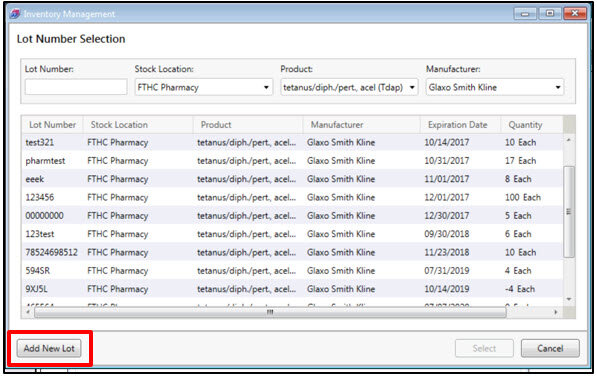
The lot number selection window will appear for you to select the Lot # associated with the medication vial
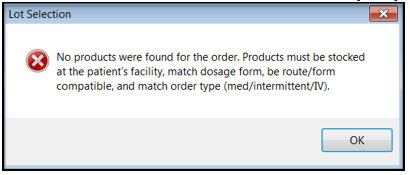
Note: If you click on the binoculars and receive the following error message, it means that the LOT for this immunization has not been added or the order does not matchthe inventory for your location
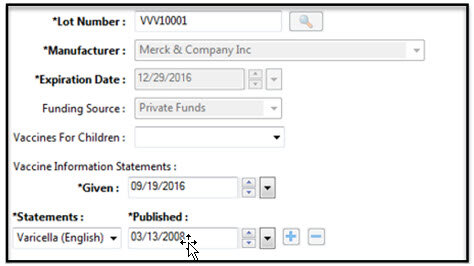
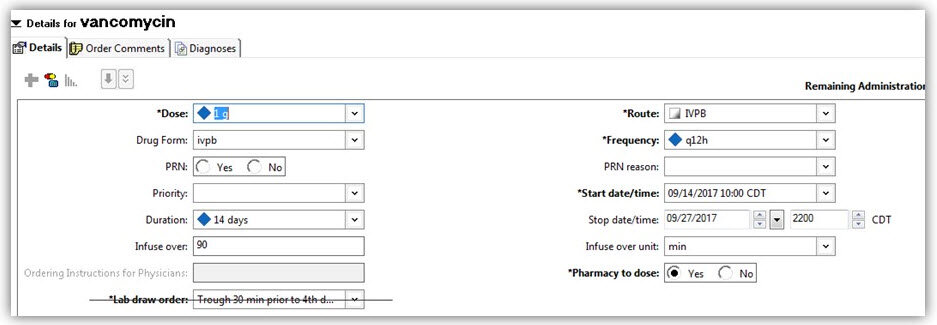
Once you select the appropriate Lot #, the maunfacturer information and expiration date associated to the alot will automatically fill in
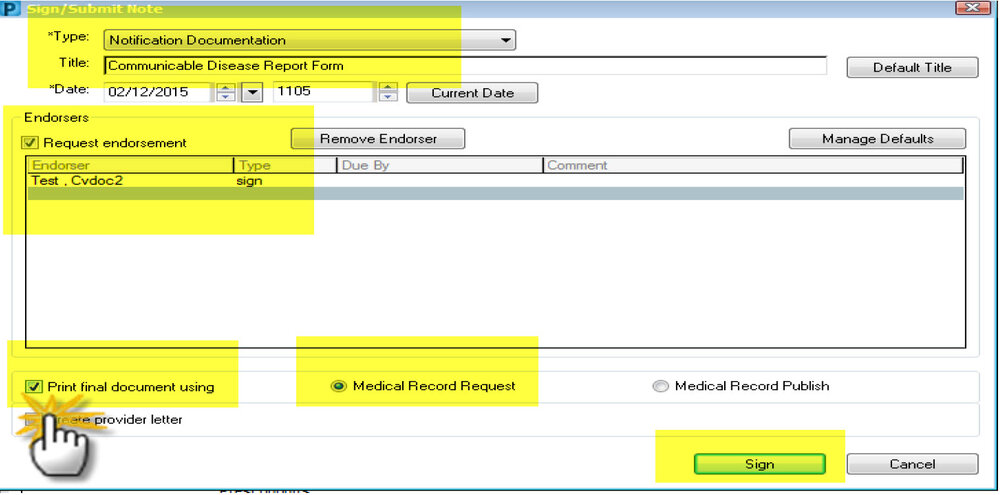
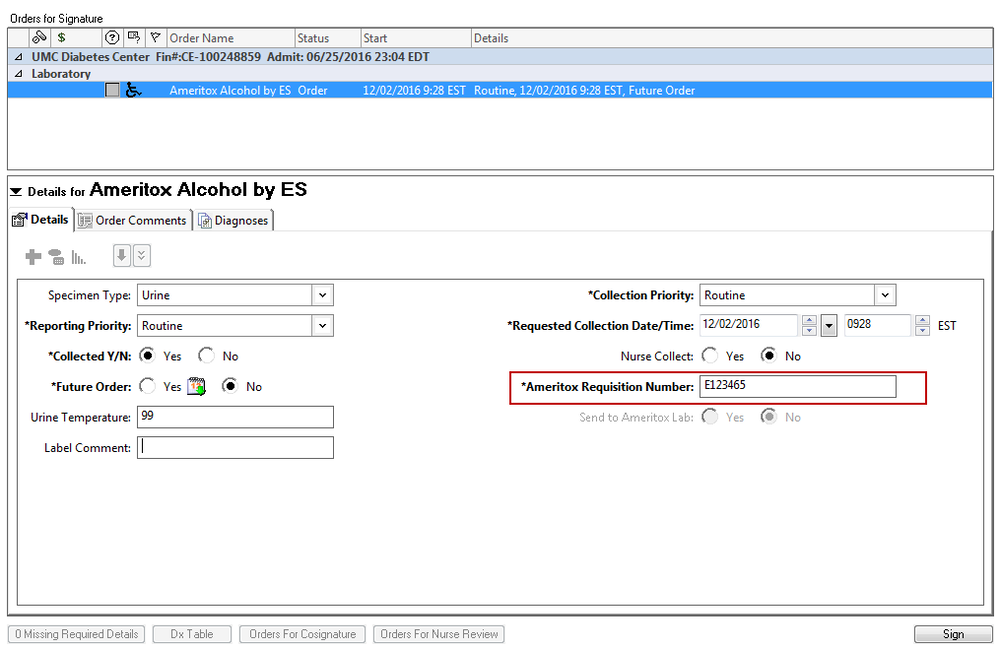
After filling out the other required fields select the Sign Documenation button and finalize the administration
Note: Shortcuts - usint the 'T' for the date fields enters the currente date; using the "N' in the time fields will enter the current time
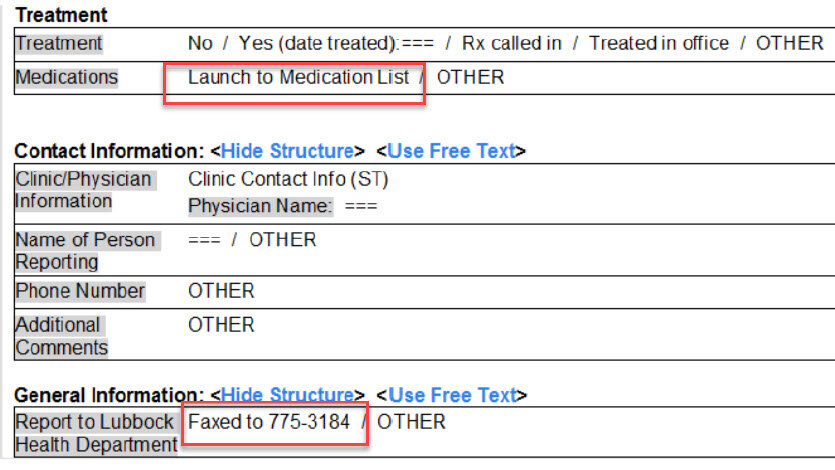
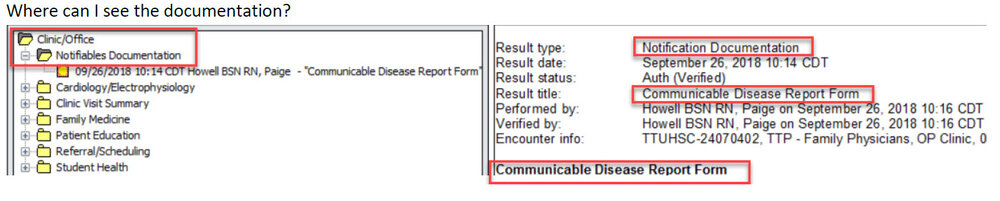
NCD Documentation:
The NDC will continue to be documetned in the Comments Field
New Lot #:
Note: This workflow is not recommeded as the typical workflow - only in situations where a Lot # has yet to be added in the MPage
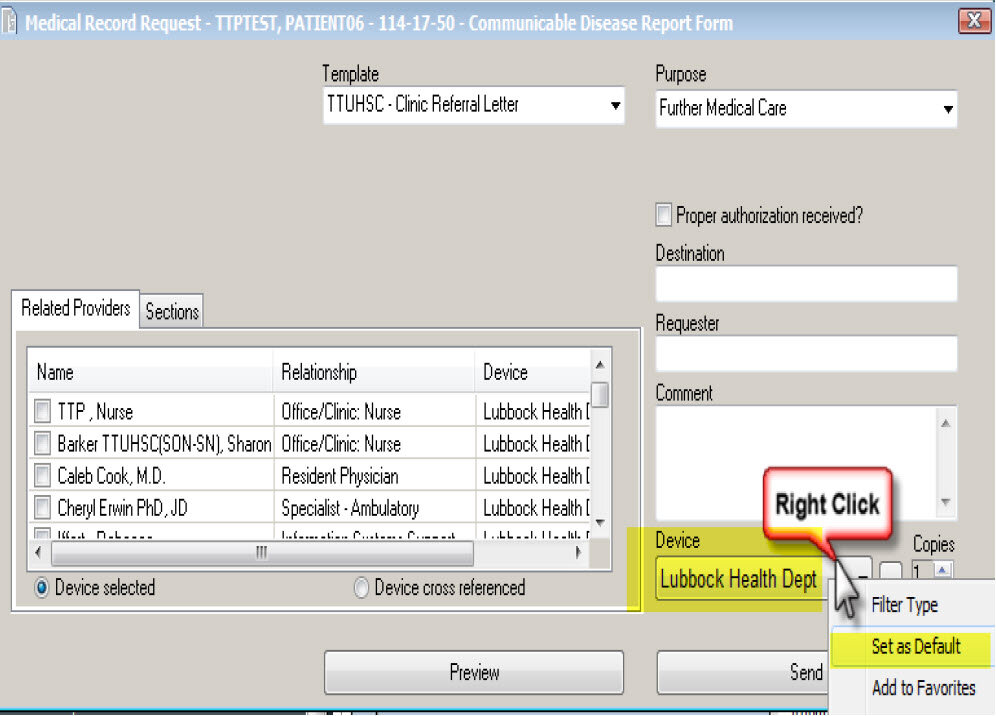
If the Lot# is not in the MPage or available within the Lot Number Selection Window > Select the Add New Lot Button at the bottom of the Lot Number Selection Window
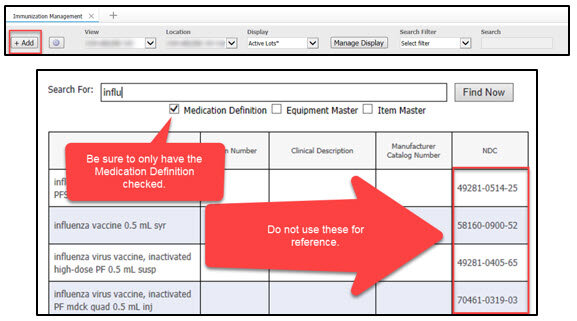
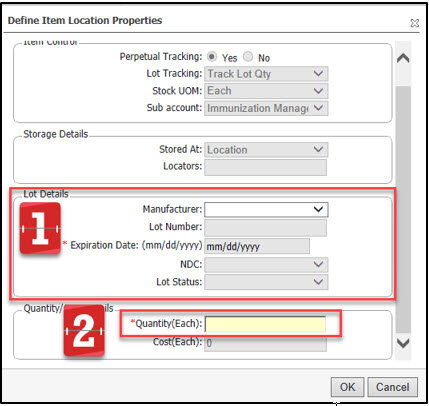
The Add Lot window will appear > enter in the required informatoin for that immunization
The Lot Number field is Case Sensitive
Enter the Lot Details within the Define Item Location Properties component
This is where the NDC will need to be verified
If the NDC is no available or needs to be updated, contact EMR Help Desk
The NDC will need to be added by the UMC Medication Management Team
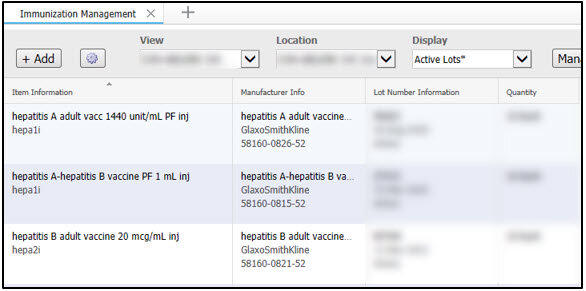
Once completed, the Immunization should appear on the selected immunization management list
Click HERE for Printable Tutorial