Changes to the medical service “Phys Med/Rehab/Wound Care” were made on December 13. The change is splitting Wound Care from Phys Med & Rehab. You can now select only Wound Care or Phys Med & Rehab within the Referral Ambulatory Order.
Dynamic Documentation Keyboard Shortcuts
Please print the printable instructions for easy access.

Changes to the Banner Bar
In January 2024, we are replacing the “High-Risk Discharge” in the Banner Bar with “Discharge Probability”.
This is to help everyone prioritize discharge planning tasks, establish early targets for discharge, and drive discussion around care progression and discharge readiness.

This value comes from CM Analytics by XSOLIS. There is a value called “p24”. This is the likelihood of discharge within 24 hours. This can be a helpful check against planned discharges and a way to identify discharge opportunities. Rare discrepancies may exist due to individual patient readiness; your clinical judgment should take precedence in those cases.
The p24 predictions are displayed as a category of likelihood (Highly Likely to Very Unlikely). Predictions falling in the middle of those ranges (Toss Up) indicate cases that require a close review for discharge readiness.
This will be discussed further as your teams meet with Dr. Amy Sikes and colleagues regarding LOS and Patient Flow.
Cerner Image Viewer
Cerner Image Viewer is a web-accessible software application that displays digital imaging as reference information to support the needs of clinicians, diagnosticians, and technologists. Image Viewer can be used for reference during patient consultations.
Changes to Procedural Sedation Note
Go-Live: November 10, 2023
Summary
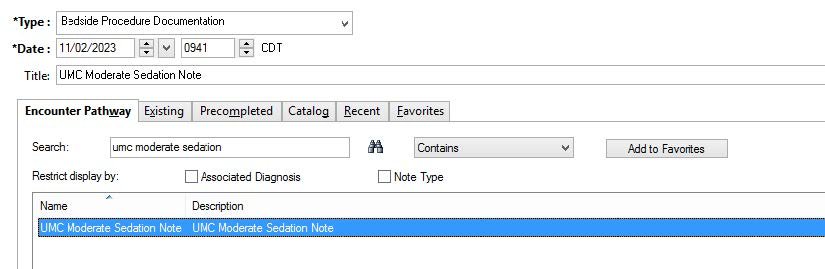
The Procedural Sedation Note has been renamed to UMC Moderate Sedation Note. This note has also been modified to meet regulatory requirements.
Where to find UMC Moderate Sedation Note
Dynamic Documentation
PICU Providers
Linked in the Dynamic Documentation Note Templates below the components.

All other Dynamic Documentation Service Lines
Search for the UMC Moderate Sedation Note from the Documentation search screen.
Choose the Bedside Procedure Documentation Note Type.

Moderate Sedation Note Autotext
In the Moderate Sedation Note, type ;moderate_sedation to populate the autotext.

PowerNote
Search for UMC Moderate Sedation Note.
The Note Type will auto-populate.
UMC Code Sepsis Note
Go-Live: November 8, 2023
Where to find UMC Code Sepsis Note
Dynamic Documentation
Internal Medicine, Family Medicine, Hospitalist, and General Surgery:
Linked in the Dynamic Documentation Note Templates below the components.

All other Dynamic Documentation Service Lines:
Search for the UMC Code Sepsis Note from the Documentation search screen.
Choose the Progress Note Type for your Service Line.

PowerNote
Search for UMC Code Sepsis Note.

Save the note under the Progress Note Type for your service line.

AMION is now an available Quick Link
UMC has added AMION as a quick link in Powerchart under the UMC Quick Links available list.

Cerner Scheduled Downtime
There will be a Cerner downtime between 12:45 AM CDT and 1:15 AM CST (approximately 1.5 hours) on Sunday, November 5th, for the fall time change. During this time, Cerner applications (PowerChart, FirstNet, SurgiNet, etc.) will NOT be available for use. Please follow the appropriate downtime procedures for your department.
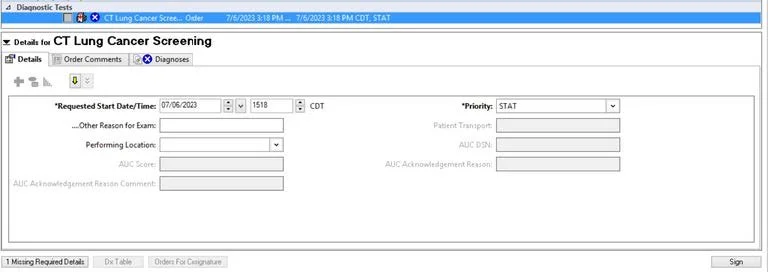
Change in LDCT Order
There has been a change to the required fields for ordering CT Lung Cancer Screening. Due to mandatory reporting requirements “Packs/Day (1 Pack = 20 Cigarettes) and “Years Smoked” have become required information in the CT Lung Cancer Screening order.

Lab Cancelation Update
In order to better communicate with providers when the laboratory cancels a lab test unexpectedly, a message will be sent to the ordering provider’s inbox in Message Center for all inpatients and outpatients (excluding ICUs) when a lab test is cancelled for the following reasons:
-Blue Top not filled properly
-Order Cancelled in Lab
-Order Entry Error
-Patient refused
-Specimen clotted
-Specimen hemolyzed
-Specimen not received
-Specimen mislabeled
-Specimen Quantity not sufficient
-Specimen Unacceptable for testing
The message will include the test name that was cancelled, the time and date the order was placed, the cancel reason, the time and date the order was cancelled and any documented communication between the lab and the nursing/clinic staff about the cancellation. Below is an example message:


Microbiology Susceptibility Update Cascade Reporting for E. Coli
Go-live: October 16, 2023
Background
Best practices dictate that de-escalation of antibiotics occur as soon as an organism is identified, and susceptibility results are available. Broad-spectrum antibiotics use in hospitals is inevitable in the era of multidrug resistance. Preferential use of narrow-spectrum agents may reduce the emergence of multidrug-resistant organisms, prevent toxicities associated with broad-spectrum agents, prevent superinfections such as Clostridioides difficile, and reduce health-care expenditure.
Cascade reporting (CR) is a less resource intensive tool that hospitals can utilize to encourage de-escalation. The Clinical and Laboratory Standards Institute (CLSI) describes Cascade Reporting (CR) as a strategy of reporting antimicrobial susceptibility test results in which secondary (i.e., broader-spectrum or costlier) agents may only be reported if an organism is resistant to primary agents within a particular drug class. There are some exceptions such as if a patient has an allergy or adverse reactions to primarily reported antimicrobial.
Each antibiotic/organism combination will follow an agreed upon cascade that is reviewed by the antimicrobial stewardship committee and approved by the pharmacy and therapeutics committee. Results that are suppressed on the antibiotic susceptibility panel are available in the microbiology lab and may be released upon request by provider (i.e., and allergy, adverse reaction, prohibited by renal or hepatic function to a released antibiotic).
The Antimicrobial Stewardship Committee and approved by pharmacy and therapeutics committee has agreed to initiate this practice with a single source and organism combination before rolling out to all sources and organisms. The initial cascade will be a urinary source growing E. coli. See below for an example:

Cascade Reporting
Background
Best practices dictate that de-escalation of antibiotics occur as soon as an organism is identified, and susceptibility results are available. Broad-spectrum antibiotic use in hospitals is inevitable in the era of multidrug resistance. Preferential use of narrow-spectrum agents may reduce the emergence of multidrug-resistant organisms, prevent toxicities associated with broad-spectrum agents, prevent superinfections such as Clostridioides difficile, and reduce health-care expenditure.
Cascade reporting (CR) is a less resource intensive tool that hospitals can utilize to encourage de-escalation. The Clinical and Laboratory Standards Institute (CLSI) describes cascade reporting (CR) as a strategy of reporting antimicrobial susceptibility test results in which secondary (i.e., broader-spectrum or costlier) agents may only be reported if an organism is resistant to primary agents within a particular drug class. There are some exceptions such as if a patient has an allergy or adverse reactions to primarily reported antimicrobial.
Each antibiotic/organism combination will follow an agreed upon cascade that is reviewed by the antimicrobial stewardship committee and approved by the pharmacy and therapeutics committee. Results that are suppressed on the antibiotic susceptibility panel are available in the microbiology lab and may be released upon request by provider (i.e., an allergy, adverse reaction, prohibited by renal or hepatic function to a released antibiotic).
The Antimicrobial Stewardship Committee and approved by pharmacy and therapeutics committee has agreed to initiate this practice with a single source and organism combination before rolling out to all sources and organisms.
The initial cascade will be a urinary source growing E. coli. See below for an example.

Lock Before You Walk
This is a friendly reminder to protect your account from unauthorized access before walking away from a computer or electronic device.
Either Tap Out with your badge
OR
Press F4
Changes to Child Life Specialist Order
Go Live: August 29, 2023
Summary
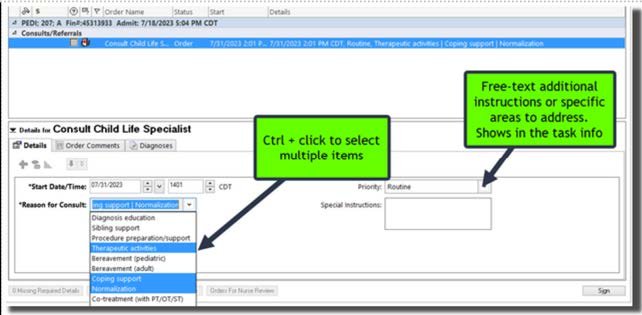
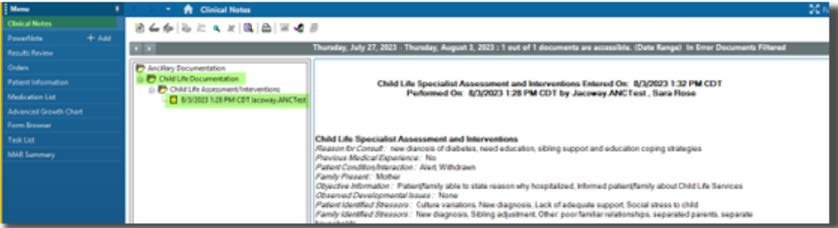
On August 29, 2023, the Child Life Specialist Order will be available with the attending physician field removed so any clinician can place the order. This order will fire a task to the Child Life Specialists' multi-patient task list containing all the details filled out in the order. The Child Life Specialist will then fill out their documentation in a Powerform that is visible to Providers in the Ancillary Documentation Folder.
Order
Child Life Specialists’ do NOT have ordering privileges, so this order must be placed by the clinician.
How to see if consult task is completed

documentation location
Provider View: Documents Component -> Change Filter to Ancillary Documentation

Clinical Notes: Ancillary Documentation Folder
Ashtma Plan Update
There has been an update made to the EC Pediatric Asthma plan. You will now see the option of adding continuous albuterol orders with the option of 250 mg/hr, inhalation-continuous, ONE TIME, x 2 hr or x 1 hr.

DFPS CPS Reporting Update
Department of Family and Protective Services (DFPS) CPS reporting process, specific to the toll-free telephone number. The details of the changes are below.
As a result of HB 63, effective 9/1/2023,
All reports of child abuse or neglect made through the DFPS toll-free telephone number are no longer anonymous
Oral reports are recorded
The reporter’s identify will remain confidential with DFPS and law enforcement
Reporters may still make anonymous reports to law enforcement
FLASH Alert: Provider Letters may be sent to a Recipient's old contact list
In the Provider Letter Recipients dialog box, Cerner has reported that old addresses, email addresses, and fax numbers may be displayed for recipients in the Recent Recipient and Favorite tabs.
Description:
This flash applies to U.S. and non-U.S. clients who use Message Center.
When you create a provider letter and select the recipients, you can select recipients from the Recent Recipient and Favorite tabs of the Provider Letter Recipients dialog box. In the Recent Recipient and Favorite tabs, the recipients' address, email address, or fax number may not be up-to-date. If you select a recipient with an old address, email address, or fax number, the provider letter may not be delivered to the correct recipient.
Impact:
Patient privacy may be impacted if the incorrect recipient receives the patient's information because a provider letter is sent to an old address, email address, or fax number. Patient care may be impacted if the correct provider does not receive the letter and the correct provider does not have information about what care the patient needs.
Resolution:
The flash does not delete the current Recent Recipient and Favorites tabs. UMC is working on cleaning up the system to ensure all recent and favorite recipients are deleted. UMC is diligently working on getting this resolved.
Coming Soon: CHANGES TO CT LUNG CANCER SCREENING ORDER
Go-Live: Mid-August
New Process:
Select the “CT Lung Cancer Screening” Order.
A form will pop up that will determine eligibility for the lung cancer screening program.
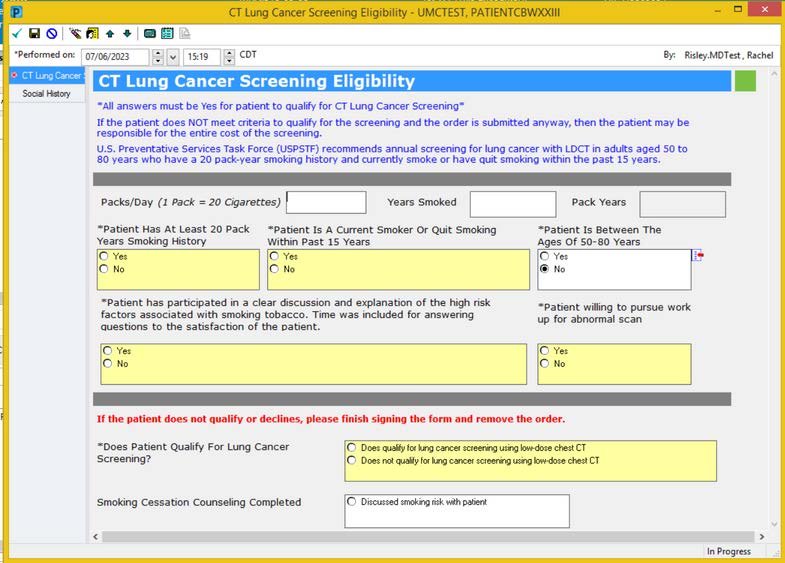
Complete and sign the form.
If this form is not completed, the order will be removed from the order scratchpad.
Complete the order details and place the order.
Plan Change: Neuro 3% Hypertonic Saline
The Neuro 3% Hypertonic Saline Protocol Plan will change to Neuro 3% Hypertonic Saline Plan. The pharmacy stated the reason below:
Please remove "protocol" from the title as this doesn't meet the IT requirements for a protocol ("Minimal clinical judgment is needed, what judgment that is needed is outlined by the protocol, otherwise provider should be contacted for assistance)... This plan should always be patient-specific and ordered/manipulated by the provider, not the nurse.
The pharmacy has also requested that the Infusion rate be changed to mL/kg/hr, and the Intermittent Dosing will remain at mL/kg/dose
New Order: Notify Provider of Urine Output
Go-Live: July 26th, 2023
This order was created to be used for urine output instead of the current Notify Provider (Misc).
It will have a required field to select “Greater than” or “Less than” and a required field for mL/hr. It will also have an optional field for any additional urine parameters.


