There have been issues identified with the "Activate All" functionality and the Oncology PowerPlans. The decision has been made to turn this functionality off.
We will remove this from all inpatient plans so that the nurse will activate individual days of treatment instead of activating all. This will help with the rescheduling of medications and days of treatment. The nurse will activate the day of treatment as she is ready to. This will follow the workflow of nursing in the outpatient setting. This will furthermore allow the outpatient chemotherapy plans we currently have built to be used in the inpatient setting.
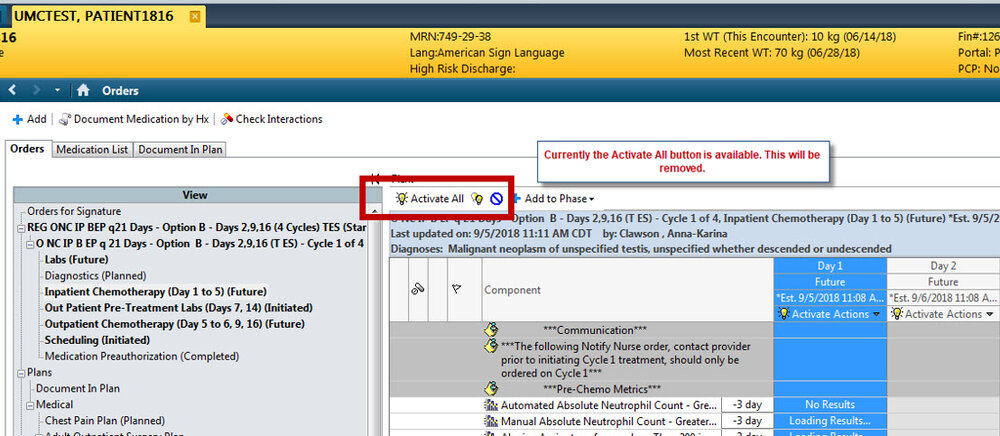
This is the current look to the Oncology Inpatient PowerPlans. The nurse clicks “Activate All” and all of the days of treatment are activated.
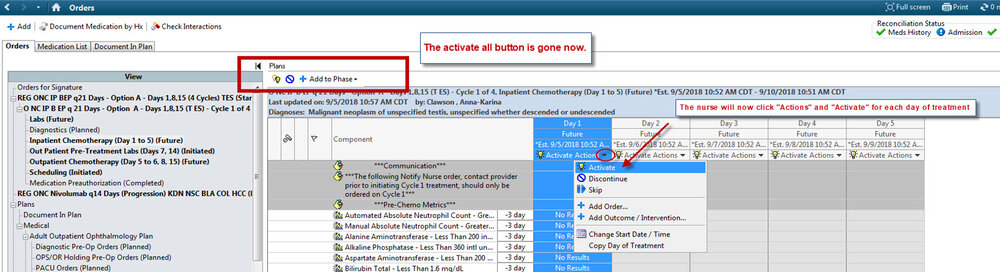
This is how it will display for the nurses. The nurses will no longer have the option to “Activate All”. They will click on the triangle next to “Actions” and click on “Activate”. This will activate the individual treatment day. In doing this, this will also allow the nurse to clearly see what day of treatment the patient should be on, especially since most of the time the same nurse does not have the same patient every day of the patient’s treatment.
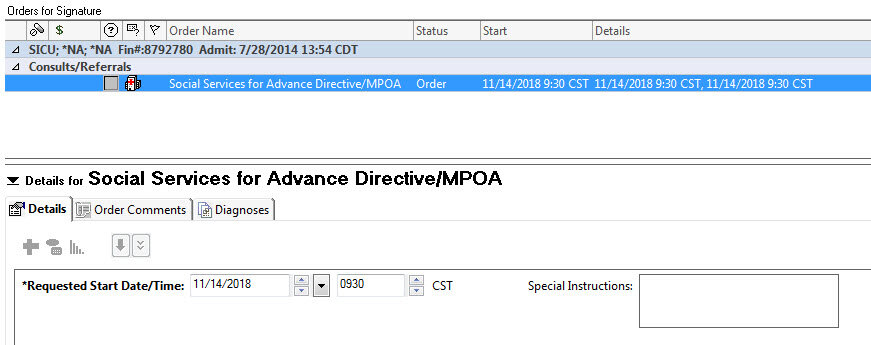
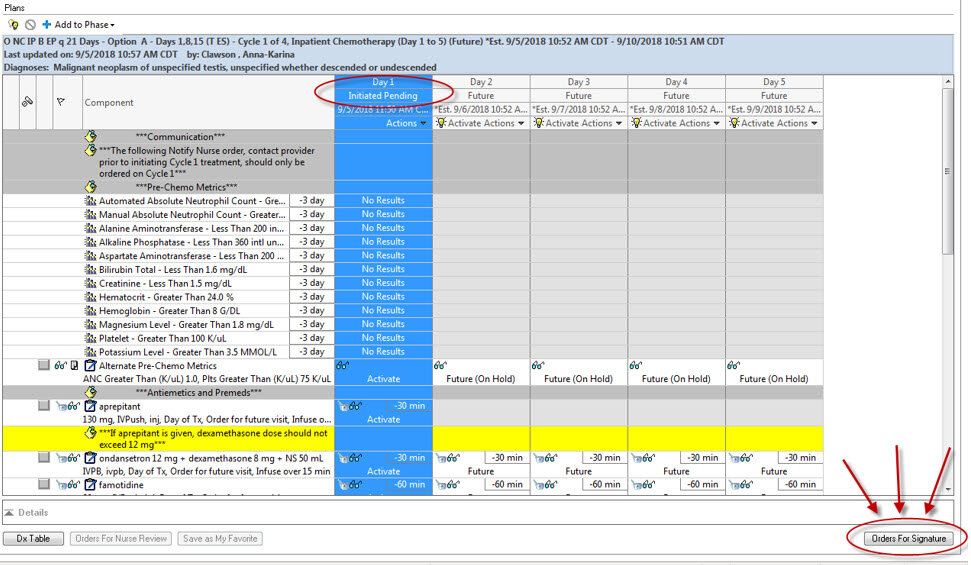
Once the “Activate” button is clicked the process is the same. The day of treatment goes into an “Initiated Pending” state. The nurses will click “Orders For Signature”
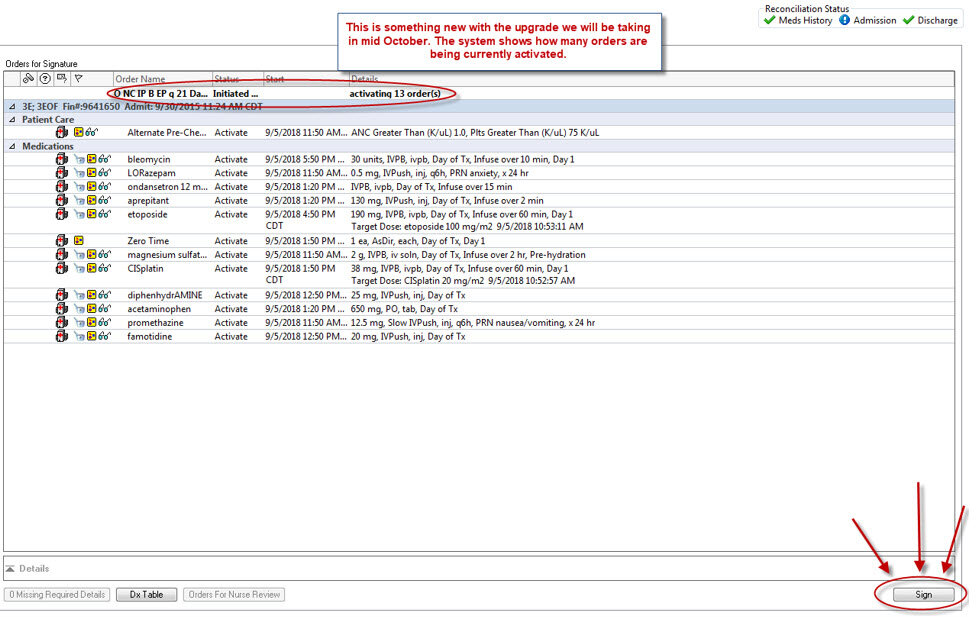
The nurses will then review the orders and click “Sign” to finish the activation process.
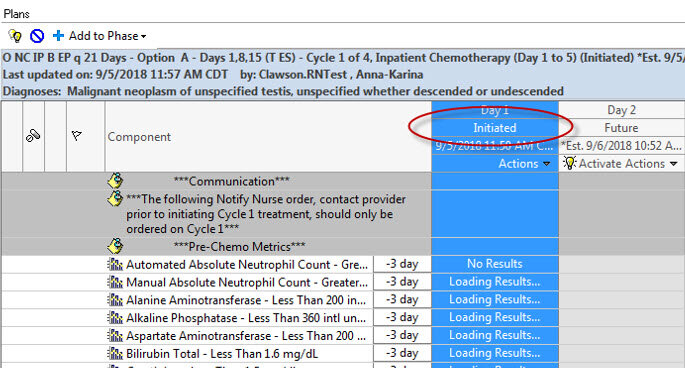
After signing, they should “Refresh” the screen. Day of treatment 1 is now in an “Initiated” status while the other days of treatment remain in a “Future” status to be activated when needed.